- About Us
- Ilizarov Technique
- Process
- Case Studies
Fractures
• Acute Fracture - Comminuted Fracture Distal Humerus - Compound Fracture & VAC • Nonunion - Proximal Tibia - Tibia - Distal Humerus • Malunion - Femur Bone Deformity
• Acute Correction
- LRS - Bilateral Tibia - LRS - Rotational Deformity Femur(with Shortening) - LRS - Oblique Plane Deformity Femur - Nailing • Ilizarov Correction - Proximal Tibia - Distal Femur • Hexapod Correction - Metaphyseal Dysplasia Bone Infection
• Infection - Femur • Infected Nonunion - Proximal Femur Joint Problems (Arthritis)
• Hip Replacement • Knee Replacement • Intra Articular Osteotomy • High Tibial Osteotomy (HTO) • Arthrolysis - Elbow • Ilizarov Hip Reconstruction - FAQs
- Testimonials



Infection - Femur
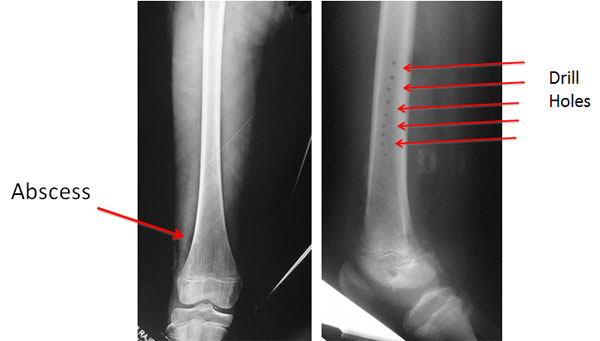
| Acute Osteomyelitis – Infection of the bone and medullary cavity is common in young children in the age group of 3-14 years. The infection presents as severe pain in the affected limb and high grade fever. This young girl of 12 years was diagnosed as acute osteomyelitis. She was treated somewhere else with I&D and Multiple drill holes. | ||
 |
||
|
||
|
||
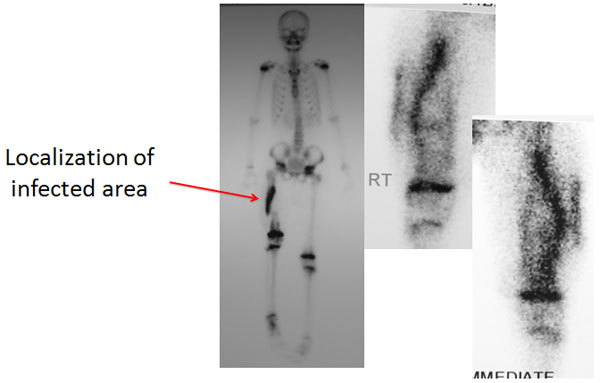
| Bone Scan | ||
| A bone scan was done which showed the area of infection. The entire shaft was infected on the inner posterior surface. | ||
 |
||
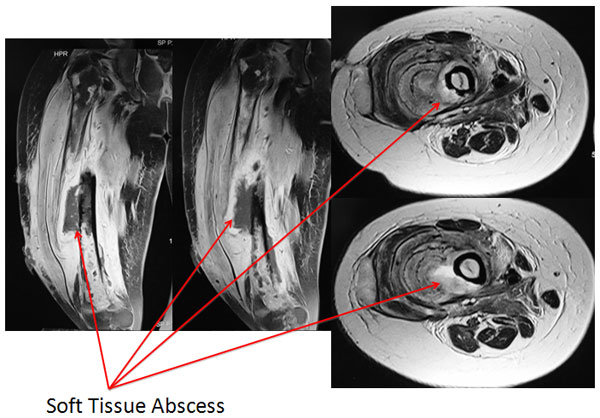
| MRI | ||
| The MRI showed a significant amount of infection in the soft tissues on the poster-lateral aspect along with the marrow infection. | ||
 |
||
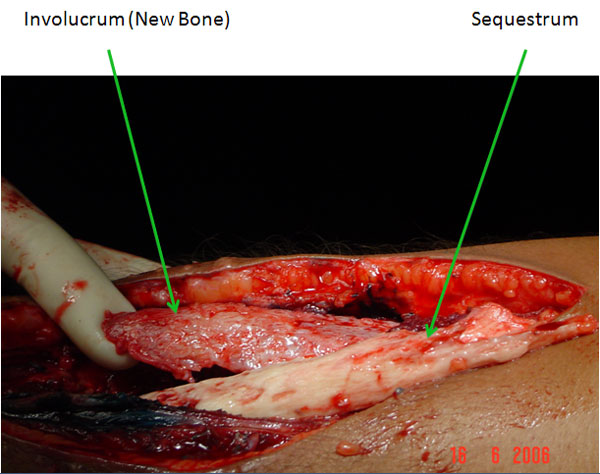
| Intra-Operative | ||
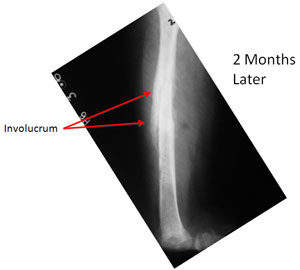
| In children with osteomyelitis, the body naturally tries to control the infection by surrounding the dead bone by new healthy bone, sort of forming a shell over the dead bone. Gradually then over a period of months to years the dead bone is then resorbed or extruded out through breaks in the skin called sinuses. The picture was taken during surgery, shows the appearance of the new bone (involucrum) – which is pink and bleeding and the dead bone (sequestrum) – which is ivory white, doesn’t bleed. | ||
 |
||
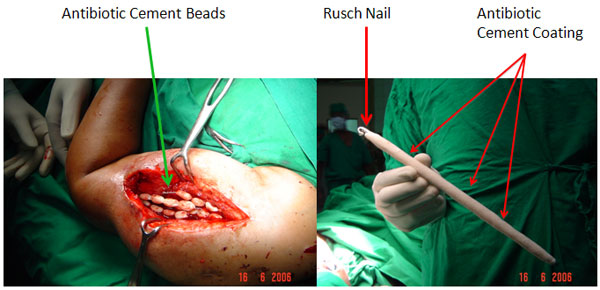
| Intra-Operative | ||
| The Picture on the left shows the placement of antibiotic cement beads in the wound. These are made during surgery using a broad spectrum antibiotic powder mixed with bone cement (PMMA). The beads are then chained on stainless-steel wires for ease of removal. The picture on the right shows the rod (Rusch Nail) on which a thick coating of the antibiotic cement is applied. The idea behind the antibiotic cement is that it allows for a slow release of the antibiotic in the local area. This creates a high concentration of the antibiotic in the local area without any associated systemic side effects. The cement allows for the leeching of the antibiotic for 4-6 weeks, by which time the infection settles down. Another advantage is the avoidance of long-term intra-venous antibiotic (Recommended duration in Osteomyelitis is about 6 weeks of IV antibiotics). | ||
 |
||
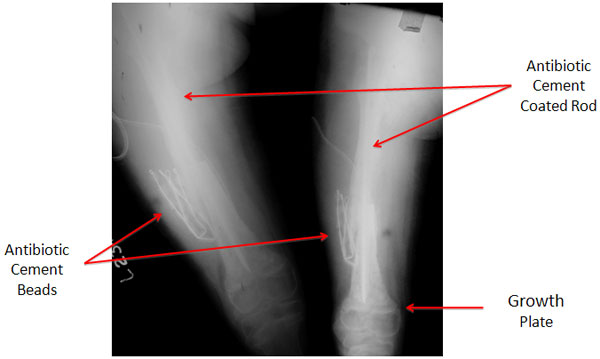
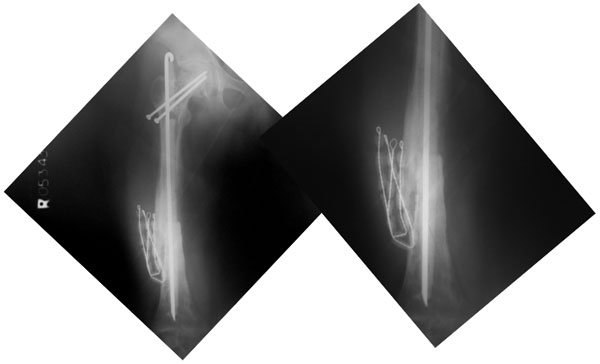
| Post Operative X-rays | ||
| The post-op x-rays showing the position of the antibiotic cement rod & beads. The fracture has been reduced after removal of the dead bone and tissue. The nail end in the lower portion of femur is just proximal to the growth plate. | ||
 |
||
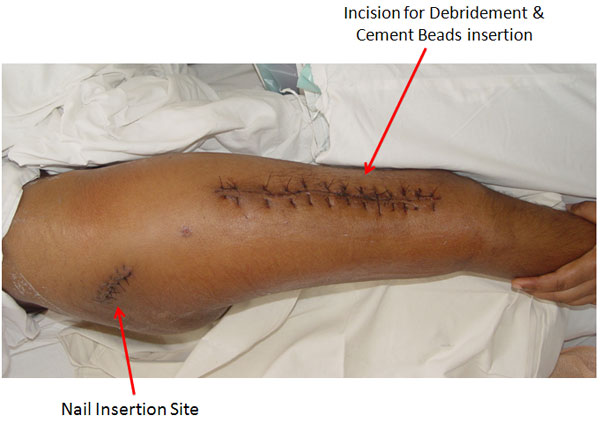
| The incision sites a few days after surgery. | ||
 |
||
| The x-rays at 2 months after surgery show good progress of healing, resolution of the infection completely and improvement in the quality of the overall bone. The screws in the neck of the femur were applied because she developed a slipped capital femoral epiphysis (slippage of the growth plate of hip joint ball). | ||
 |
||
| 5 Months Post Op | ||
| The X-ray pictures 5 months after the surgery. These were actually taken prior to removal of the antibiotic cement beads. The fractures have healed well, the infection is also settled, with no signs of recurrence and no signs of loosening of the implants. | ||
 |
||